Nilocas - Stenosis Detection
Coronary artery stenosis, a common form of heart disease is the narrowing and partial blockage of the arteries supplying the heart muscle by fatty or calcified plaques. Coronary Heart Disease is estimated to affect 250,000,000 people worldwide and is one of the world's single biggest killers [1]. Diagnosis is expensive and time-consuming, particularly because the gold standard is coronary angiography, requiring invasive catheterisation of patients under radioactive X-ray guidance. What’s more, half of those patients who undergo this testing do not have coronary artery stenosis [2].

A development by Queen Mary University London (QMUL), Nilocas is a less invasive, wearable diagnostic device to detect coronary artery stenosis. The device requires no radiation dose, can be used by less specialised staff and in any setting.
In doing so, Nilocas will offer cheaper, quicker, and safer detection.
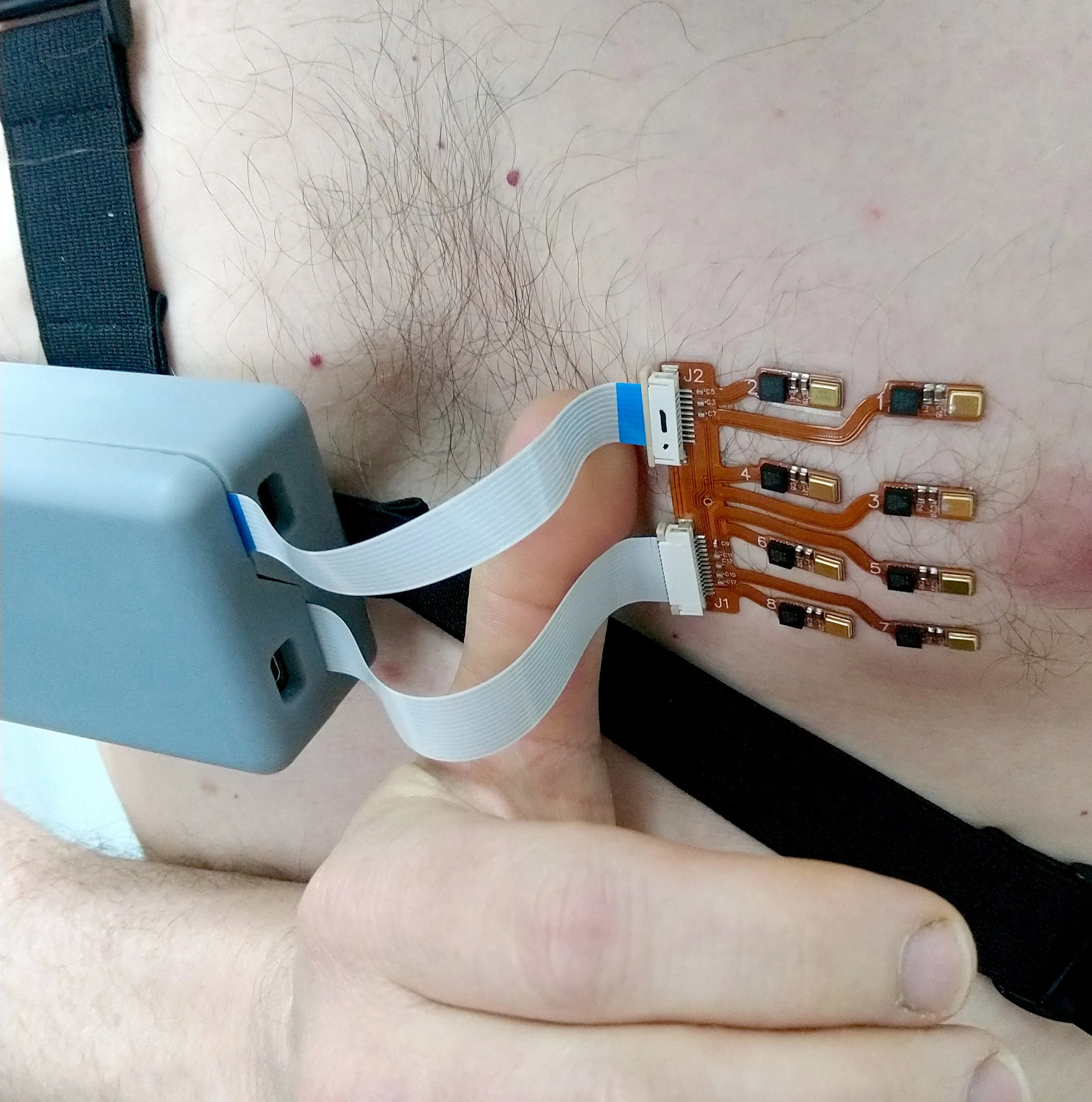
With Nilocas, an array of miniature accelerometers and microphones on a flexible printed circuit board (PCB) listen through the skin to the disruption of blood flow caused by a blockage. Signals are amplified and broadcast wirelessly for real-time interpretation by researchers.

While our engineers collaborated with QMUL to optimise and version their existing hardware build, they outlined potential future hardware improvements, and our design team conceived the possible longer-term realisation of the device.
Beginning with the existing build of PCBs which were used for in vitro testing on a simulated chest, the immediate aim was to update the wearable hardware to make it suitable for in vivo testing with human participants.

The flexible PCB patch with the accelerometer and microphone sensor array was redesigned to separate the sensors out. This increased its overall mobility improving adhesion to the flexible, dynamic surface of skin; and so reducing disruption to the signal.


The new wearable hardware retains the existing PCB designs but with the wireless transmitter enclosure at a 20% reduced volume and manufactured in appropriately accredited prototype material. A number of other design revisions were made to optimise performance and to facilitate the reduction in enclosure size including updating the antennae, switches and battery components.


The sensor patch is connected to the transmitter enclosure via ribbon connectors. Once the optimal length was determined with simple prototype rigs, more compliant wires were sourced to reduce the deferred load from the enclosure to the patch that could cause it to detach.

A range of initial weighted prototypes were tested to determine a comfortable and secure strap configuration across the anatomy of both sexes and a range of body types.
These straps are attached to the wearable enclosure via a simple bracket with keyway fixings. This approach meant the straps could be fitted and comfortably secured, then the device attached once the straps are in place. Additionally, those parts in direct contact with participants could be readily removed for cleaning or replacement.


In August, the results of the in vitro testing were presented at the MBIE Conference by Prof. Steve Greenwald, demonstrating the possibility to detect different flow rates and stenosis severities. In vivo testing is underway, using the hardware Designworks developed and built.
Parallel to redesigning and updating the hardware, our engineers defined proposals for the next development of the device. After supporting the initial steps of numerous university spin-outs requiring staged development funding, we’ve found it good practice to be looking ahead in this way. These plans include updating to edge digitising sensors for improved signal integrity, further component updates to reduce the wearable’s scale, and defining anticipated data flow to support the AI inference that Nilocas plan for later stages.
Looking farther ahead still, our designers envisaged how the technology could exist at scale in a point-of-care rather than a research context. The vision is a system that is intuitive and easy for a health care professional to use, with a small disposable carrier that is discarded for the device to be quickly cleaned and turned around ready for the next use.


An innovative placement feature on the disposable was devised to help locate the ideal location over the wearer’s heart, and an interface was designed with simple controls and graphical user interface (GUI) to indicate progress and remaining test time.
Integrating the sensor array, controls and GUI all into a single enclosure should reduce the amount of relative movement of different parts, so minimising disruptive noise. The use of edge digitising sensors should streamline the front-end processing to facilitate a smaller envelope, making the device more comfortable and less intrusive to wear.



Upon completion of the current in vivo testing, we’re hoping Nilocas will be able to return with insights and further requirements to help accelerate the journey of the device towards primary care use, where it can provide vital early detection of stenosis.
[1] British Heart Foundation Global Heart and Circulatory Diseases Fact Sheet, 2024